Prescribing in Perinatal Mental Health: Guidance for general practitioners (GPs) and Prescribers in primary care.
In pregnancy and the post-natal period, many mental health problems have a similar nature, course, and potential for relapse as at any other times. However, there can be differences; for example, bipolar affective disorder type one with at least a 1 in 4 (1,4) risk of post-partum psychosis, compared to 1 in 500 (2) in the general population.
Depression and anxiety are common mental health problems and can affect 15-20% (3) of women in the first year after childbirth. Anxiety disorders can worsen, GAD (Generalized anxiety disorder) PTSD (Post traumatic stress disorder) and OCD (obsessive compulsive disorder) can exist on their own or with depression. For many this will be their first episode of mental illness and first baby.
Shame, fear of being judged or being dismissed by professionals can mean a delay in seeking help and receiving treatment. This can have adverse consequences immediate and long term not just for the woman but the infant, the mother-infant relationship, fathers, and families. Suicide remains the leading cause of maternal death one year post-delivery and depression the most common diagnosis
(7,8).
Affective disorders of severe unipolar and bipolar affective disorder are at risk of relapse and postpartum psychosis. Psychosis can re-emerge or be exacerbated in pregnancy and the post-natal period. Some women are at higher risk of post-partum psychosis, those with previous postpartum psychosis, bipolar type 1, schizoaffective disorder, or women with no past illness but a mother or sister who has had postpartum psychosis (1,4). Post-partum psychosis can also occur in women with no previous history. (1,4)
There is a high risk of relapse in the early postpartum period in women across the whole spectrum of severe mental illness. Discussions with women and their partners about this risk and continuation of prophylactic medication during pregnancy and the post-partum period is important if we are to reduce this burden of illness and save lives. (3,6-8)
Decisions around medication in the perinatal period should involve an individual risk benefit analysis to the likelihood of relapse and discussions with the woman, partner, family, or carer about treatment options and particularly concerns about the foetus or baby. (3,6)
NICE (National Institute for Health and Care Excellence) clinical guideline for antenatal and post-natal mental health (CG192) recommend that information should be provided about:
• the potential benefits of psychological and psychotropic treatments,
• possible consequences of no treatment,
• possible harms associated with treatment,
• what might happen if treatment is changed, stopped, particularly if psychotropic medication is stopped abruptly.
This guideline is aimed at the busy GP to provide a resource summarising current information about psychotropic medication to aid the above discussion. It is not comprehensive but hopefully provides relevant information set out in an accessible way. The Royal College of General Practitioners have the Perinatal Mental Health Toolkit which is a helpful resource Perinatal Mental Health Toolkit
(https://www.rcgp.org.uk/clinical-and-research/resources/toolkits/perinatal-mental-healthtoolkit.aspx).
-
• Avoid stopping or switching psychotropic abruptly simply because a woman is trying to conceive, is pregnant or breastfeeding.
• Do not aim to reduce medication in late pregnancy to reduce neonatal withdrawal. This increases risk of relapse at a time when relapse is most likely to occur.
• Remember babies need well mothers.
• Use medication with the lowest risk profile while considering the mother’s previous response to treatment.
• Choose a medication that a woman is known to respond well to. This is likely to be the safer option. The risk of relapse and/or deterioration in mental health usually outweighs the risk of harms to foetus.
• There are risks associated with any medication; discuss this with woman and family.
• Use the lowest effective dose possible of medication but avoid subtherapeutic doses.
• Avoid polypharmacy.
• There are no absolutes.
• If unsure contact the SMABS (Specialist Mother and Baby Mental Health Service’s) perinatal adviceline via email: perinatalsmabs@bdct.nhs.uk Please note that this is non-urgent advice and will be triaged by the duty worker will review the client records and if needed liaise with a medic in the team, before getting back to you. *
• When starting a psychotropic medication in any woman of childbearing age consider the possibility her becoming pregnant at any point in the future; discuss this with the patient.Women who are on mood stabilisers should be referred to the Perinatal Mental Health Service (SMABS) for pre-conception counselling or when pregnant. **
* Section 9 Perinatal Mental Health Referral Pathway and Perinatal Advice Line (SMABS) ** Section 8 SMABS Specialist Mother and Baby Mental Health Service referral criteria
-
We understand GPs are very experienced in prescribing anti-depressants in primary care. We aim to summarise guidance and help aid conversations with patients when discussing depression and anti-depressants.
NICE (National Institute for Health and Care Excellence) clinical guideline for Depression (CG90)9 summarises the key points to discuss when taking a history from a patient presenting with depression. The important things to note are:
• History of mental illness,
• what was the response to psychotropic medication in the past?
• What happened if/when medication was stopped in the past?
• What was/is the impact on daily life when they were unwell?Choice of antidepressants
Antenatal and postnatal depression has shown to have adverse outcomes for the foetus, mother and wider family. It is generally agreed the risks and effects of poor mental health during the antenatal and postnatal period, outweigh any possible adverse outcomes of treatment with antidepressants. There are no absolutes and treatment must be tailored to the individual woman.
• Where a woman has taken antidepressants before choosing an antidepressant that is known to be effective for the woman.
• When starting an antidepressant in a woman with no previous antidepressant use or where she has responded to more than one SSRI (Selective serotonin reuptake inhibitors) choose Sertraline because it has the lowest amount passing in breastmilk.
• Use therapeutic treatment doses and the lowest effective dose for that woman.
• Continue and adjust the dose as needed in pregnancy and postnatally as risks of depression increases in the postnatal period.
• Avoid polypharmacy.Psychological therapies
NICE (National Institute for Health and Care Excellence) clinical guideline for antenatal and post-natal mental health (CG1923 recommend psychological intervention as a first choice in the perinatal period. For those with mild to moderate anxiety and depression without significant history, psychological therapies alone may be sufficient. However, women who are known to previously suffer, or are currently experiencing moderate to severe anxiety or depressive illness may well benefit from both psychological intervention and antidepressant medication.
Women who are pregnant or have a baby under one year old are fast-tracked for psychological therapies. The NICE guidance recommend perinatal women are offered an assessment within two weeks and treatment within four weeks. The woman may self -refer or be referred by a health professional to My Wellbeing IAPT via Single Point of Access (SPOA). Preconception
SSRIs (Selective serotonin reuptake inhibitors) are not known to reduce fertility, however impaired libido and sexual dysfunction may occur. Refer women with a history of severe mental health illness to secondary services for pre-conception counselling.
In early pregnancy
• The primary risk of miscarriage increases with age.
• Taking SSRI antidepressants in early pregnancy is not associated with increased risk of miscarriage or birth defects.
• Being mentally well, before, during and in the postnatal period is good for both mother and baby. Babies need well mothers.In later pregnancy
Babies, when born, may experience neonatal adaptation syndrome that is self-limiting and requires no specific treatment. Babies present with irritability, crying, shivering, increased tone, feeding and sleeping difficulties. If present onset is 8 -48 hours and fade by 72 hours. Neonatal adaptation syndrome is possibly more common with Venlafaxine than SSRI’s.
Persistent pulmonary hypertension of the new-born (PPHN) can cause serious breathing difficulties to the new-born. PPHN affects one in 500 babies (0.2%) in the general baseline population. In mothers taking SSRIs there is a small statistically higher risk of one in 333 babies (0.3%). A recent meta-analysis suggested that it is probably due to confounding factors rather than a direct result of the SSRI medications. This medication alert to the neonatology team is important, so they will be aware of the potential risk and will check the baby.6,10,11
Learning and behaviour
Evidence about possible link with Autistic Spectrum Disorder (ASD) and Attention Deficit Hyperkinetic Disorder (ADHD) is not conclusive. No causal link with SSRIs has been made due to confounder of genetics and the impact of mother (or fathers) depression itself. 6
Scientific studies have also suggested that having untreated depression during pregnancy may increase the risk of learning and behavioural problems, including ASD, and lower IQ, in the child. This is thought to be a result of the effects that depression may have on how a mother is able to interact with her baby. 6
Antidepressants in breastfeeding
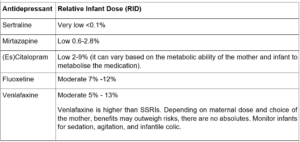
Generally, the benefits of breastfeeding outweigh the risks if the infant is full term and healthy. If premature, consult with a paediatrician. Monitor infants for sedation and poor feeding. Relative Infant Dose (RID) less than 10% is considered safe. The amount in breastmilk is much less than the amount infant is exposed to in-utero and breastfeeding can reduce neonatal adaptation syndrome.6
See the table below listing the RIDs for common antidepressants used based on LactMed 23 database.
-
Preconception
Some antipsychotics, such as Risperidone and Amisulpride, can increase prolactin and make it harder to get pregnant.
If a woman taking antipsychotics is finding it hard to conceive, check her prolactin levels.
If this is high, investigate to exclude other causes and refer to secondary mental health team to consider switching to an antipsychotic less likely to raise prolactin such as olanzapine, quetiapine and aripiprazole 12. There is a risk of relapse when switching antipsychotics, so it is important to monitor mental state for any changes. Alternatively, if a switch is not appropriate, the secondary mental health team may consider adding adjunctive low-dose aripiprazole to normalise prolactin levels (note: polypharmacy should generally be avoided – assess the risks and benefits)30.During pregnancy
Pregnancy is not protective against psychotic episodes in women with schizophrenia. Schizophrenia is associated with adverse outcomes for the mother and baby 6. Generally, the risk of not treating psychosis outweighs the risk of adverse outcomes due to treatment.
A pregnant woman who is stable on an antipsychotic and is likely to relapse without medication should continue antipsychotic medication 3.
Dose adjustment may be necessary, particularly in the later stages of pregnancy due to increased drug clearance and subtherapeutic concentrations 13. Closely monitor patients for change in mental status and adjust antipsychotic dose if appropriate. The minimum effective dose of an antipsychotic should be prescribed.
If a woman decides not to take medication during pregnancy, consider re-starting the antipsychotic within 24 hours of birth to lower the risk of postpartum psychosis 12.
Note: data regarding the safety of antipsychotics in pregnancy and the postnatal period is limited.Risks of harm to baby
Antipsychotics are not associated with adverse maternal outcomes or an increase of birth defects. There is most reproductive safety data available for quetiapine, olanzapine, risperidone and haloperidol 14.
There is an increased risk of gestational diabetes and weight gain with olanzapine, quetiapine and clozapine 15.
All pregnant women on antipsychotics should be monitored for gestational diabetes and excessive weight gain. Offer oral glucose tolerance test between 24 and 28 weeks of pregnancy. If they have had gestational diabetes before, offer oral glucose tolerance test earlier in pregnancy and again at 24-28 weeks if the first test is normal 16. Discuss healthy eating guidance.Clozapine
Clozapine may be used in pregnancy, but this must be under the supervision of secondary care services. If there are any changes in smoking habits, dose adjustment and plasma level monitoring should be considered.
Depot Antipsychotics
Depot can be continued when a pregnant woman is responding well to a depot and has a history of non-adherence with oral medication 3.
Postpartum
Neonatal withdrawal
Neonatal withdrawal may occur (e.g., crying, agitation, increased suckling). This is usually mild and self-limiting. When antipsychotics are taken in pregnancy, it is recommended that the woman gives birth in a unit that has access to paediatric intensive care facilities (2). Breast feeding may minimise withdrawal symptoms.6
Breastfeeding
Generally, the benefits of breastfeeding outweigh the risks if the infant is full term and healthy. If premature, consult with a paediatrician.
Babies breastfed by a mother taking antipsychotics should be monitored closely due to case reports of drowsiness, irritability, motor abnormalities and poor feeding 6.
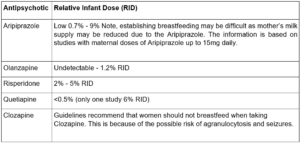
All antipsychotics pass into breastmilk, usually in small amounts; the amount of drug which passes to the baby through breastmilk is lowest for olanzapine and quetiapine. However, babies may still be breastfed even when the mother is on other antipsychotics.
Aripiprazole can reduce prolactin levels and result in mothers not being able to produce enough breast milk to exclusively breastfeed.
Clozapine is contraindicated in breastfeeding women due to the risk of neonatal agranulocytosis and seizures 12.See the table below listing the RIDs for common antipsychotics used based on LactMed 23 database:
-
Antipsychotics Olanzapine, Quetiapine and Aripiprazole have a better risk/benefit profile in pregnancy and breastfeeding and should be considered first-line treatment for the treatment of bipolar affective disorder in women of child-bearing age. (3,6) Where first-line treatments have proved ineffective; a woman may require a mood stabiliser continued as maintenance and prophylaxis treatment in pregnancy and postpartum psychosis or relapse (5,17).
Preconception
Refer women on Lithium and other anti-epileptic drugs or pre-conception Counselling (see appendix 1). Discussions with specific information about her individual likelihood of relapse, treatment options and particularly concerns about baby, help women and their partners decide what is best for them and the baby. This may be to a decision to remain on the mood stabiliser, stop gradually and monitor or switch to another medication such as an antipsychotic, prior to conceiving.(3,6)
Lithium
Preconception
Lithium is prescribed for the treatment of bipolar affective disorder type one, schizoaffective disorder, and/or recurrent depression where an antidepressant alone has failed. If antipsychotics with a safer risk profile have proved ineffective, the benefits may outweigh the risk of harm to baby, of continuing Lithium.
Risk of harm to baby
There has been specific concern about a mother taking Lithium in early pregnancy increasing the risk of heart defects in babies. The heart is fully formed by 8 weeks of pregnancy. 1 in 100 babies is born with a heart defect ranging from mild, moderate to severe – even when a mother has not taken medication. (6,18)
The increased risk associated with taking Lithium in the early weeks of pregnancy is much lower than previously thought. (6,19-21) Current studies (19,20) estimate a risk of one additional case per 100 live births.
There was a concern that a rare heart problem Ebstein anomaly that occurs in 1 in 20,000 babies – even where no medications has been taken. The original study in the late 1970’s was flawed in its conclusions and included women taking not only Lithium but also teratogenic anti-epileptic medications. (6,22) Recent large registry studies (19-21) have not found an association with Lithium and the risk of Ebstein anomaly, if present, is extremely small. (6,19-21)
Given the cardiac malformation risk is much lower than previously thought it is important that the benefit of maternal mental illness and the risk of serious post-partum illness is considered. This risk is particularly high if a woman is not taking medication.
• Refer to the specialist perinatal service SMABS for per-conception counselling with a perinatal psychiatrist, or if already pregnant as soon as possible, to weigh the individualised risks pre-conception and the options. The need of close and careful Lithium monitoring of Lithium levels through pregnancy, labour and postpartum can be explained. Lithium levels need to be monitored monthly in pregnancy then weekly from 36 weeks and birth should take place in hospital.
• Refer to the specialist perinatal service SMABS any woman pregnant of Lithium, or who may have stopped Lithium to become pregnant, as soon as you become aware. She must be managed in secondary mental health services, with a perinatal psychiatrist and consultant obstetric care. (3,6,18,22)Breastfeeding
It is recommended not to breastfeed on Lithium, Lithium passes freely into the breastmilk and there are risks of toxicity to neonate. The Lithium levels in breastmilk fluctuate widely with Relative Infant Dose (RID) of up to 45.
Sodium Valproate
Preconception
This drug is absolutely contraindicated in pregnancy and should also not be prescribed to any female of child-bearing potential unless absolutely necessary and the conditions of the pregnancy prevent programme (24) are met. If prescribed, the rationale for this must be clearly documented and the patient (and if appropriate the parents) must be aware of the risk to the baby.
Women of childbearing age taking Valproate must have a yearly review with the appropriate specialist (neurologist or psychiatrist) and complete the risk acknowledgement form. (24) This to show that the above conditions have been met and everyone understands the risks of becoming pregnant while taking Valproate.
Risk of harm to baby
There is a high risk of Valproate harming babies in the womb.
10% of babies born to mothers taking Valproate in pregnancy will have a birth defect.
– Spina bifida, facial or skull malformations, abnormalities to the limbs, heart, kidney, urinary tract and sexual organs
40% of babies born to mothers taking Valproate in pregnancy will have developmental difficulties.
– Delayed walking, speaking, lower intelligence, poor speech and language skills, poor memory.
– Children exposed to valproate in the womb are more likely to have autism or autistic spectrum disorders. There are also some evidence children may be more likely to be at risk of developing symptoms of attention deficit hyperactivity disorder (ADHD).The Medicines and Healthcare products Regulatory Agency MHRA (UK) has produced various documents to support healthcare professionals and patients around valproate prescribing and can be found online Valproate use by women and girls – GOV.UK (www.gov.uk). (24)
Pregnancy
Do not stop Valproate suddenly as this could trigger a relapse. (6,25) Refer to a Perinatal Psychiatrist in the perinatal mental health service, together with the woman it can be decided what medication would be safest in pregnancy and postnatally.
• Refer to the specialist perinatal service SMABS any woman pregnant on Valproate, or who may have stopped Valproate to become pregnant, as soon as you become aware. She must be managed in secondary mental health services with consultant-led obstetric care. (3,6)
Carbamazepine
Carbamazepine should not be started in women planning a pregnancy or pregnant. The decision to continue Carbamazepine in pregnancy requires an individualised risk benefit discussion between the woman and her prescriber. Carbamazepine is linked to an increased risk of neural tube defects and birth defects. The risk however smaller than Valproate (6,26). More studies are needed. If she is prescribed Carbamazepine as a mood stabiliser.
• Refer to the specialist perinatal service SMABS for per-conception counselling with a perinatal psychiatrist, or if already pregnant as soon as possible, to weigh the individualised risks pre-conception and the options in pregnancy and postnatal.
• If carbamazepine is prescribed for neurological condition, urgent referral to the neurologist is recommended.Lamotrigine
The current evidence does not suggest it is a major teratogen. Babies when born or breastfed may develop apnoea, drowsiness, poor sucking, and rash. Lamotrigine is found in high levels in breastmilk. Infant serum levels should be checked to rule out toxicity, as well as monitoring of platelet count and liver function.23
If she is prescribed Lamotrigine as a mood stabiliser:
• Refer to the specialist perinatal service SMABS for per-conception counselling with a perinatal psychiatrist, or if already pregnant as soon as possible, to weigh the individualised risks pre-conception and the options in pregnancy and postnatal.Folic acid supplementation
Folic acid supplementation is recommended in pregnancy. While this should continue to be offered to women taking anti-epileptic drugs, it is worth noting that evidence for valproate does not suggest that supplementation prevents birth defects or malformation.
-
Promethazine
Promethazine is usually the first choice for short-term use in insomnia. There is a good amount of data showing that promethazine is not linked to an increased risk of malformation. To reduce the risk of discontinuation symptoms and side-effects in the baby, the dose of promethazine may need to be reduced or stopped before the woman’s due date. Promethazine passes into breast milk in small amounts, but a woman can still breastfeed if the baby is healthy and full term. (27)
Benzodiazepines
NICE guideline does not recommend using benzodiazepine in the perinatal period, and if it is used it should be clearly defined the indication, the length of the treatment, and the lowest possible dose should be given. Mothers should be educated about breastfeeding, not recommended, especially higher doses, co-sleeping is also not recommended.
Benzodiazepines are used for their sedative and relaxant properties, they differ in their potency, time of onset and duration of action. Although some studies have found an association between benzodiazepines and congenital malformations, many studies do not support benzodiazepines being teratogens. Many of the studies that supported the association between benzodiazepine and congenital anomalies had not controlled for confounding factors such as indication, concomitant medications, or substance use disorders, recent maternal illness, and maternal age. It would therefore be beneficial to consider these factors before prescribing. (28)
• Diazepam (long acting) crosses the placenta and could potentially accumulate in foetal tissue and in the breastfed infant.
• Lorazepam (short acting) crosses the placenta less readily, and new-borns can clear lorazepam.
• The use of shorter acting agents, such as lorazepam and oxazepam is generally preferred and where possible to be used short-term, intermittent dosing to reduce infant exposure. (28)Possible complications with benzodiazepine use include preterm delivery, low-birth weight, low Apgar score, floppy baby syndrome, neonatal intensive care unit admission and respiratory distress syndrome, motor, or mental development, however they have not been consistently supported. (27)
Zolpidem
Zolpidem is short-acting and is said to clear from the foetus quickly, though placental passage varies greatly. (28)
Zopiclone
Zopiclone; little information is known about its use in pregnancy, and it’s not recommended in breastfeeding due to its long half-life. (27) There isn’t much data on the levels of these drugs in breast milk and safety in breast-feeding. Recommendations in many reference texts are often based on a small number of case reports. (29)
NICE recommends that these drugs only be used short-term, if considered necessary for extreme anxiety and agitation. (3)
-
Substance misuse in pregnancy is linked to many poor maternal and foetal outcomes. Women should be stabilised on substitute medications or discontinued before pregnancy, but if this is not possible their use should be limited. Refer women to the local substance misuse service (CGL/New Directions) for support. Once referred, women who are pregnant are fast-tracked by CGL and prescribed substitutions as soon as possible. Midwives and other teams are also involved to provide specialist care during this time.
-
The Specialist Mother and Baby Mental Health Services (SMABS) is specialist secondary perinatal mental health team within Bradford District Care NHS Foundation Trust serving Bradford and Airewarfe and Craven. We are a 9am to 5pm Monday to Friday service for women who are at high risk of severe perinatal mental illness or experiencing moderate to severe mental illness in pregnancy and in the postnatal year.
SMABS email: perinatalspecialistt@bdct.nhs.uk
SMABS’s clients and referrals in process: SPA 01274 221180
Useful perinatal mental health information: https://bdct.sharepoint.com/sites/PerinatalMentalHealth
GP’s, health visitors, midwives, obstetricians as well as mental health professionals can share concerns, seek advice and consultation, and discuss possible referral with a member of the SMABS team 08:30 to 16:30 Monday to Friday. Due to agile working and COVID we now operate this via the SMABS e-mail address with a return phone call rather than a direct telephone adviceline. We aim to respond within one working day but for all urgent matters please contact First Response.
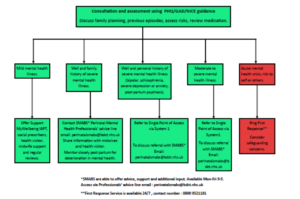
Consider referring a woman to secondary mental health services, specialist perinatal mental health service SMABS for preconception counselling if she has a current or past severe mental health problem (postpartum psychosis, bipolar affective disorder type one, schizoaffective disorder, schizophrenia, psychosis or severe depression especially if associated with psychosis) and is planning a pregnancy, or if she as a high-risk woman and pregnant, even if she is currently well.
Consider referring a woman to secondary mental health services, specialist perinatal mental health service SMABS for preconception counselling on mood stabilisers Lithium, Sodium Valproate or any anti-epileptic drug prescribed as a mood stabiliser.
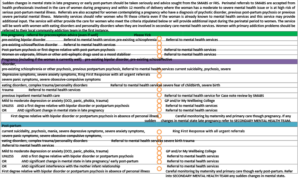
Consider referring a woman to secondary mental health services, specialist perinatal mental health service SMABS who is experiencing current suicidality, psychosis, severe depressive symptoms, severe anxiety symptoms, severe panic symptoms, severe obsessive-compulsive symptoms, eating disorders, complex trauma, severe birth trauma, in pregnancy or the post-partum.
All routine referrals to secondary mental health services including specialist perinatal mental health services to be made via the Single Point of Access (SPOA).
Ring First Response 0800 952 1181, 24 hours 7 days a week, for all urgent referrals. Suspected post-partum psychosis is an emergency because it can escalate in a matter of hours, current suicidality, psychosis, severe depression, and severe anxiety.
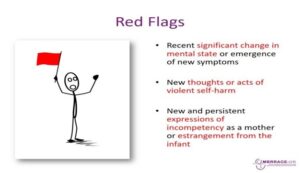
Perinatal women are prioritised and where there are red flag presentations; First Response aim to provide a 4-hour response as per NICE guidance.
It is worth knowing that access to IAPT (Improving Access to Psychological Therapies) psychological therapies for women who are pregnant or in the first postnatal year is now fast-tracked – two weeks to assessment and four weeks to treatment. Psychological interventions should be offered first-line to women with mild to moderate anxiety and depression as per NICE.
-
Appendix 1- SMABS Referral Criteria
-
About perinatal mental health:
• Perinatal Mental Health Toolkit for GPs https://www.rcgp.org.uk/clinical-and-research/resources/toolkits/perinatal-mental-healthtoolkit.aspx
• Mind: Perinatal Mental Health https://www.mind.org.uk/information-support/types-of-mental-health-problems/postnataldepression-and-perinatal-mental-health/about-maternal-mental-health-problems/
• Mind: www.mind.org.uk/information-support/drugs-and-treatments/
Medication information in pregnancy and breastfeeding:
Information leaflets for professionals and patients about individual medications
• Best Use of Medications in Pregnancy (BUMPS) : www.medicinesinpregnancy.org
• Choice and Medication : www.choiceandmedication.org
• Antipsychotics in pregnancy and breastfeeding: https://www.rcpsych.ac.uk/mentalhealth/treatments-and-wellbeing/antipsychotics-in-pregnancy
• Valproate in women and girls who could get pregnant: https://www.rcpsych.ac.uk/mentalhealth/treatments-and-wellbeing/valproate-in-women-and-girls-who-could-get-pregnant
• Lithium in pregnancy and breastfeeding: https://www.rcpsych.ac.uk/mentalhealth/treatments-and-wellbeing/lithium-in-pregnancy-and-breastfeedingProfessionals
• UK Teratology Information Service http://www.uktis.org/
• LactMed for breastfeeding: Drugs and Lactation Database (LactMed) – NCBI Bookshelf (nih.gov) or download the LactMed App -
1. Munk-Olsen T et al. Risks and predictors of readmission for a mental disorder during the postpartum period. Archi Gen Psychiatry. 2009 Feb; 66(2):189-95
2. VanderKruik R et al. The global prevalence of postpartum psychosis: a systematic review. BCM Psychiatry.2017;17:272
3. National Institute for Health hand Care Excellence (2014) Antenatal and post-natal mental health: Clinical management and service guidance. NICE Guidelines CG192. www.nice.org/guidance/cg192
4. Chadalavada B et al, Postpartum psychosis for carers. Royal College of Psychiatrist. Oct
2018
Postpartum Psychosis for Carers | Royal College of Psychiatrists (rcpsych.ac.uk)
5. Wesserloo R et al. Risk of postpartum relapse in bipolar disorder and postpartum psychosis: a systematic Review and Meta-analysis. Am J Psychiatry, 2016; 173: 117-127
6. Hamish McAlister Williams R et al, British Association of Psychopharmacology consensus guidance on the use of psychotropic medication preconception, in pregnancy and postpartum, 2017;31:519-552, Available at: https://www.bap.org.uk/pdfs/BAP_GuidelinesPerinatal.pdf
7. Saving Lives, Improving Mothers’ Care MBRRACE-UK 2015. M Knight et al
8. Saving Lives, Improving Mother’s Care MBRRACE-UK 2017. M Knight et al
9. National Institute for Health hand Care Excellence (2009) Depression in adults: recognition and management. NICE Guidelines CG90 https://www.nice.org.uk/guidance/cg90
10. Medicinesinpregnancy.org. 2022. USE OF SERTRALINE IN PREGNANCY. [online]
Available at: <https://www.medicinesinpregnancy.org/bumps/monographs/USE-OFSERTRALINE-IN-PREGNANCY/>
11. Masarwa, R., Bar-Oz, B., Gorelik, E., Reif, S., Perlman, A. and Matok, I., 2019. Prenatal exposure to selective serotonin reuptake inhibitors and serotonin norepinephrine reuptake inhibitors and risk for persistent pulmonary hypertension of the new-born: a systematic review, meta-analysis, and network meta-analysis. American Journal of Obstetrics and Gynecology, 220(1), pp.57.e1-57. e13.
12. Royal College of Psychiatrists. Antipsychotics in pregnancy. Available at:
https://www.rcpsych.ac.uk/mental-health/treatments-and-wellbeing/antipsychotics-inpregnancy
13. Westin, A. A. et al. (2018) “Treatment with antipsychotics in pregnancy: Changes in drug disposition,” Clinical pharmacology and therapeutics, 103(3), pp. 477–484.
14. Taylor, D. M., Barnes, T. R. E. and Young, A. H. (2021) The Maudsley prescribing guidelines in psychiatry. 14th ed. Hoboken, NJ: Wiley-Blackwell 15. Betcher, H. K. and Wisner, K. L. (2020) “Psychotropic treatment during pregnancy: Research synthesis and clinical care principles,” Journal of women’s health (2002), 29(3), pp. 310–318.
16. National Health Service (2019). Gestational diabetes. Available at:
https://www.nhs.uk/conditions/gestational-diabetes/
17. Viguera A C et al, Risk of recurrence of bipolar disorder in pregnant and nonpregnant women after discontinuing lithium maintenance, Am J Psychiatry 2000; 157:179-184
18. Windsor L et al, Lithium in Pregnancy and Breastfeeding. Royal College of Psychiatrist. Oct 2018 Lithium in pregnancy and breastfeeding | Royal College of Psychiatrists (rcpsych.ac.uk)
19. Patorno E et al, Lithium use in pregnancy and the risk of cardiac malformations. N Engl J Med 2017; 376:2245—2254
20. Munk-Olsen T et al, Maternal and infant outcomes associated with lithium use in pregnancy: an international collaborative meta-analysis of six cohort studies; Lancet Psychiatry 2018 Aug; 5(8):644-652
21. Boyle B et al, The changing epidemiology of Ebstein’s anomaly and its relationship to maternal mental health conditions: A European registry-based study, Cardiol Young 2016;677-685
22. Poels EM et al, Lithium during pregnancy and after delivery: a review Int J Bipolar Disorder 2018;6:26
23. LactMed,2022. Drugs and Lactation Database (LactMed). [online] Ncbi.nlm.nih.gov. Available at: https://www.ncbi.nlm.nih.gov/books/NBK501922/
24. Valproate use by women and girls – Information about the risks of taking valproate medicines during pregnancy. (Published March 2018, Updated Feb 2021). Valproate use by women and girls – GOV.UK (www.gov.uk)
25. Strachan G, Valproate in women and girls who could get pregnant, Royal College of Psychiatrist, Oct 2018 Valproate in women and girls who could get pregnant | Royal College of Psychiatrists (rcpsych.ac.uk)
26. Matlow J and Koren G, Is Carbamazepine safe to take in pregnancy? Can Fam Physician. 2012 Feb; 58(2): 163–164.
27. Lian Chua. Prescribing in women Medics teaching. Specialist Mother and Baby Mental Health Service Bradford. March 2021
28. Simriti K. Chaudhry et al. Considerations in Treating Insomnia During Pregnancy: A Literature Review. Department of Psychiatry, Hospital of the University of Pennsylvania, Philadelphia, PA. Psychosomatics, 2018; 59(4): 341-348.
29. Perinatal Mental Health: Prescribing Guidance for Trust Prescribers and GPs. Dr Jenny Cooke et all. West Sussex partnership NHS Foundation trust. October 2019; 5.
30. Mypsych.nhsggc.org.uk. 2022. Antipsychotic combination/augmentation. [online] Available at: <https://mypsych.nhsggc.org.uk/medicines-companion/antipsychotics/antipsychoticcombinationaugmentation/#:~:text=The%20optimum%20dose%20of%20aripiprazole%20for %20managing%20symptoms, may%20have%20a%20detrimental%20impact%20on%20me ntal%20state> [Accessed 10 March 2022].